8:00 a.m -6:00 p.m
-
-
-
RMZ Ecoworld, Bellandur, Outer Ring Road
8:00 a.m -6:00 p.m
RMZ Ecoworld, Bellandur, Outer Ring Road
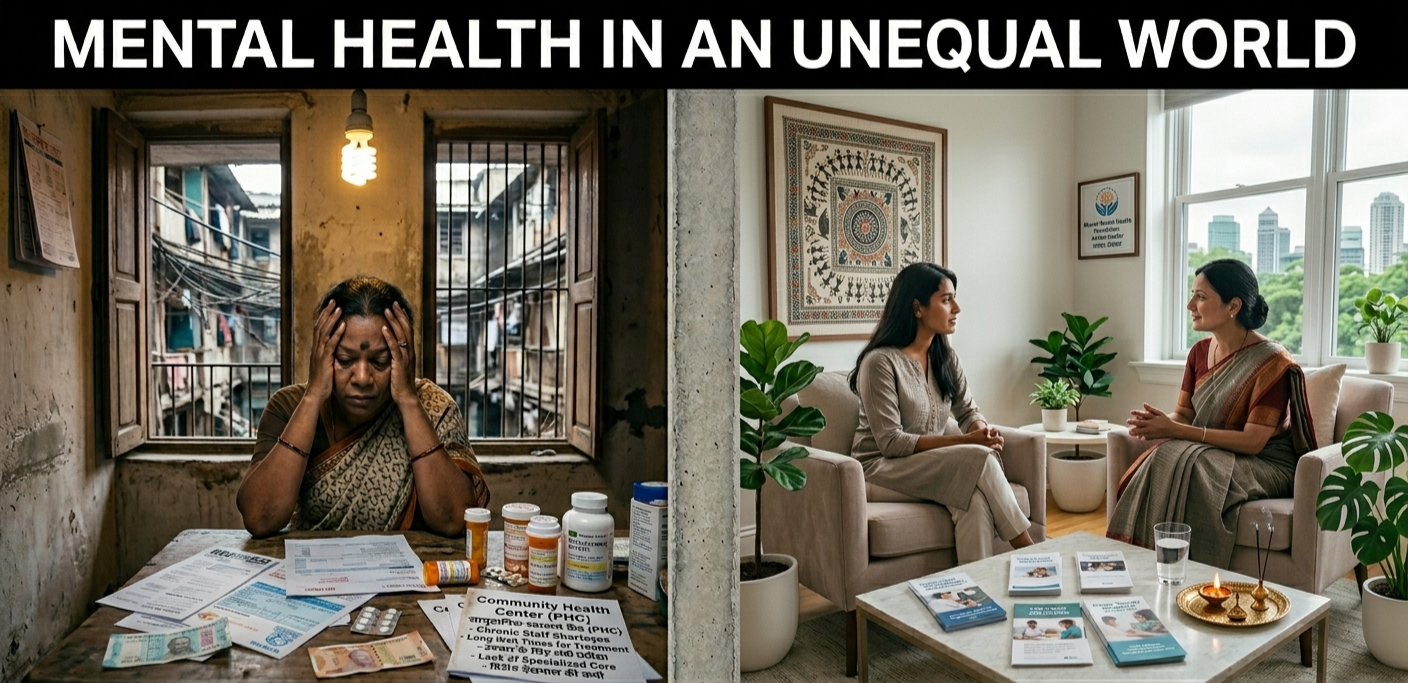
Where you are born, how much you earn, whether you are a man or a woman, the colour of your skin, the language you speak — none of these should decide whether your mind gets the care it needs. And yet, around the world, they do. This is the hard truth behind the idea of mental health in an unequal world: good mental health is not shared out fairly. The people who face the most hardship in life often carry the heaviest mental load, while having the least access to support.
At Manushee, we see this every day in the women who come to us. So let's talk honestly about what drives these gaps, why they matter, and — most importantly — what each of us can do about them.
The phrase first reached a global audience as the theme of World Mental Health Day 2021. Marked every year on October 10th and led by the World Federation for Mental Health, that year's theme was chosen by a worldwide public vote. The message was simple but powerful: mental illness does not strike at random. The risk of mental health problems rises and falls with the conditions of a person's life.
We all have mental health, just as we all have physical health. Anyone, in any home or any income bracket, can struggle. But the chance of developing a mental health condition — and the chance of getting help for it — is shaped by forces far larger than any single person. Researchers call this mental health inequity: the unfair and avoidable gap, between different groups of people, in both the risk of mental illness and access to mental health care. In an unequal world, your postcode and your pay slip can matter as much as your biology.
The scale of this is hard to overstate.
Globally, close to one billion people were living with a mental disorder even before the COVID-19 pandemic — and the pandemic pushed rates of depression and anxiety up by around 25%. Mental health conditions are now among the leading contributors to the global burden of disease, responsible for one in every six years a person lives with disability. Suicide accounts for more than one in a hundred deaths worldwide, and most of those deaths happen before the age of 50.
Yet the response remains small. On average, countries spend only about 2% of their health budgets on mental health, and just 7% of global health research funding goes towards the mind. In some countries there are as few as two mental health workers for every 100,000 people. The result is a treatment gap so wide that, in some places, up to 90% of people who need care receive none.
And the burden is not evenly spread. Around 82% of people living with a mental health condition are in low- and middle-income countries — the very places with the fewest resources to help. This is what social inequity looks like when it reaches the mind.
India shows this inequality in sharp relief. The National Mental Health Survey of India (2015–16) found that nearly 15% of adults — roughly 150 million people — need care for one or more mental health conditions. But the treatment gap ranges from about 70% to over 90% depending on the disorder, sitting at roughly 83% overall. In plain terms: most Indians living with a mental illness never receive formal treatment.
Geography deepens the divide. Around 70% of Indians live in rural areas, yet most mental health services, specialists and hospitals are clustered in cities. For a woman in a remote village, the nearest psychiatrist may be a day's travel and a month's wages away. Often, traditional healers or faith leaders are the first — and sometimes only — point of contact.
Why should something as social as income or discrimination affect something as personal as the mind?
The answer lies in what experts call the social determinants of mental health — the everyday conditions in which we are born, grow, live, work and age. Insecure work, unsafe housing, debt, discrimination, loneliness and violence are not just unpleasant; they are chronic stressors. Over months and years, they keep the body's stress response switched on, slowly wearing down both mind and body.
This is why hardship and mental illness so often travel together, and why the relationship runs both ways. Poverty raises the risk of mental health problems — and mental health problems can deepen poverty through lost work, medical costs and social exclusion. It becomes a cycle that is hard to break alone. Sometimes the weight is even older than we are, carried across generations as patterns of stress and survival passed quietly from parents to children.
At Manushee, we take this seriously. The chronic stress that follows people through unequal lives is not a character flaw — it is a physiological reality, and it can be treated.
Inequality is never only about money. Several overlapping forces shape who is most at risk.
Income and poverty.
There is a clear social gradient in mental health: the lower a person sits on the economic ladder, the higher their risk of distress. Financial strain, job insecurity and debt are among the most powerful predictors of poor mental wellbeing.
Gender
Women carry a distinct and often invisible mental load. Globally, women experience higher rates of depression and anxiety than men, for reasons that are deeply social: a greater burden of unpaid care work, higher exposure to domestic and sexual violence, and norms that ask women to hold families together while putting their own needs last. In India the picture is starker still — the country ranks among the lowest in the world for gender equality in health and survival, and has one of the highest female suicide rates globally. The hormonal transitions across a woman's life — from menstruation to pregnancy and the postpartum period to menopause — add another layer that is too often dismissed rather than treated.
Caste, ethnicity and race.
Discrimination — whether open hostility or daily micro-aggressions — is a chronic stressor that raises the risk of depression and anxiety. Marginalised communities also tend to receive poorer treatment and to trust services less.
Sexual orientation and gender identity.
People who are lesbian, gay, bisexual, transgender or queer consistently report poorer mental health than their heterosexual peers — not because of who they are, but because of the stigma, harassment and exclusion they face.
Geography and age.
Rural communities, older adults, refugees and displaced people are all more likely to experience social isolation, and less likely to find nearby, affordable care.
Most people don't fit neatly into one box. A poor, rural woman from a marginalised community faces these pressures stacked on top of one another — what researchers call intersectionality — which is exactly why support has to see the whole person, not a single label.
Even when someone recognises they need help, a wall of barriers can block access to mental health services:
Cost
Therapy and medication are expensive, and insurance rarely covers mental health the way it covers physical health.
Stigma
In many communities, mental illness is still seen as weakness, moral failing or shame. In India, stigma is the single most common reason people give for not seeking help — fearing harm to their marriage, job or family standing.
Distance and workforce shortages
Too few professionals, concentrated in too few cities, leave vast areas effectively uncovered.
Culturally insensitive care.
Services that don't speak a person's language or understand their world can fail to recognise distress, or turn people away.
This is why the unmet need for mental health care is often even greater than the unmet need for physical health — even in wealthy countries.
COVID-19 did not create these inequalities, but it exposed and deepened them. Lockdowns brought job losses, grief and social isolation, and the heaviest blows fell on those already struggling. Women lost work and absorbed more caregiving; frontline and informal workers had little protection; young people lost schooling and connection. The pandemic was a shared storm — but, as many have observed, we were not all in the same boat.
None of this is inevitable. Inequality is, in large part, a set of choices — and choices can be remade. Real progress works at the individual and societal level at once, on three fronts.
Governments can invest far more than 2% of health spending in mental health, fold mental health care into primary health systems, and tackle the root causes — poverty, insecure work, violence and discrimination. Promoting mental wellbeing for all is written into the United Nations' Sustainable Development Goals, a reminder that this is a shared global commitment rather than a luxury.
Care works best close to home. Community health workers, peer supporters with lived experience, and local healing circles can reach people that clinics never will — especially in low- and middle-income countries, where evidence shows trained non-specialists can deliver genuinely effective support.
Every conversation that treats mental health as real, ordinary and worthy of care chips away at stigma. Reaching out for help is not weakness; it is one of the bravest and most practical things a person can do.
You cannot single-handedly fix global inequality. But you can protect your own mind, and you deserve to. A few places to start:
• Name what's yours and what isn't. Much of the stress in an unequal world comes from circumstances, not from any failing in you. That distinction alone can ease a lot of shame.
• Protect your foundations. Sleep, movement, nourishing food and time outdoors are not indulgences. They are the ground your mental health stands on.
• Stay connected. Social isolation is one of the strongest risks to wellbeing. A regular call, a walk with a friend, or a support group can be genuinely protective.
• Treat your stress load as information. If worry, low mood or exhaustion are becoming hard to manage, that is a signal to act — not a sign of failure.
• Ask for help early. The sooner support begins, the easier recovery tends to be. You do not have to wait for a crisis.
The idea of mental health in an unequal world can feel heavy, even hopeless. But understanding the forces at work is the first step to loosening their grip — and no one should have to carry that weight alone.
At Manushee, we built a women's-only space for exactly this reason. We know that women's mental health is shaped by pressures the world too often ignores, and our holistic, evidence-based and trauma-informed approach is designed to meet women where they are, with compassion rather than judgement. Whether you are living with anxiety, depression, grief, or the long shadow of trauma, our SAFE programme is here to help you regulate mind and body safely.
If you are ready to take the first step, you can book a free discovery call and meet our team. A more equal world starts with making sure your mind gets the care it deserves.